Glioblastoma (GBM) patients are known to have a poor prognosis and tumor progression with high mortality and a median survival of only 12-15 months. Currently, anti-GBM therapy includes a multi-modality method involving radiotherapies and surgical removal of the tumor in combination with chemotherapy.1
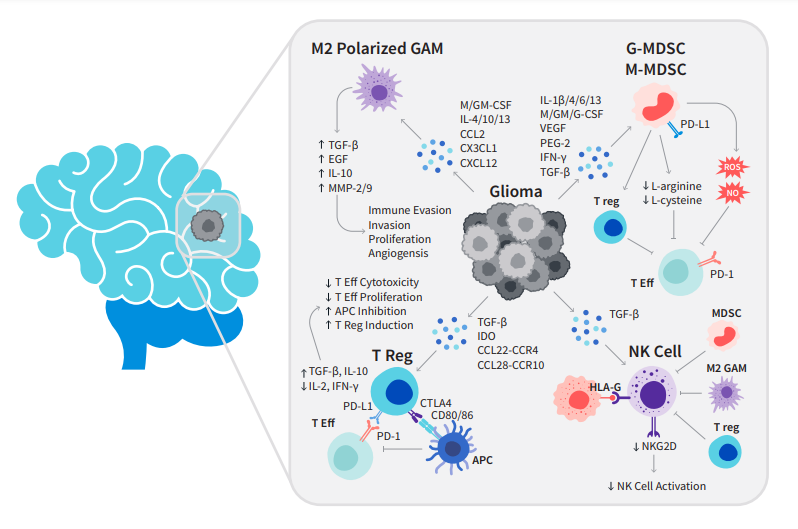
Unfortunately, these tumors can often be resistant to radiotherapy as well as chemotherapy and surgical removal of the entire tumor may not be possible.1 New immunotherapy drugs may provide an alternate approach to treatment, aiming to bolster the immune system to eradicate disease. However, GBM is a highly complex disease with limited effective treatment options because of its highly angiogenic nature and its notorious ability to suppress the immune system both locally at the tumor and systemically in the body (Fig. 1).1,2 The brain being an immune-privileged tissue poses challenges in addition to the blood-brain barrier that further limits our therapeutic options such as the use of antibody therapies.1 However, investigation of immuno-oncology drugs may overcome this limitation as one may only need the immune cells to cross the blood-brain barrier. In addition, targeting the mechanisms by which glioma cells evade destruction by the immune system may allow us to provide patients with a meaningful survival benefit.2