Introduction
Multiple myeloma is a hematological malignancy that arises from antibody-producing plasma cells that is rarely detected prior to symptomatic disease onset. Multiple myeloma was the cause of nearly 100,000 deaths worldwide in 20181 and it is estimated that in 2021, approximately 35,000 new cases of multiple myeloma will be diagnosed and cause 12,500 deaths United States2.
Multiple myeloma takes up residence and produces lytic lesions in the bone marrow – in addition to death from tumor progression, multiple myeloma lesions result in bone pain, fracture, anemia, and kidney dysfunction as a result of paraprotein production by malignant plasma cells that can cause damage to other organs.
There are several clinically approved therapeutics for the treatment of multiple myeloma with diverse mechanisms of action, including cyclophosphamide (DNA alkylating agent), bortezomib and carfilzomib (proteasome degradation blockade), and doxorubicin (DNA intercalation). There are also approved therapies that target aspects of the immune system, including daratumumab and isatuximab (CD38 targeting monoclonal antibodies)3. Many of these therapies are either approved or under clinical investigation to be used in combination with one another.
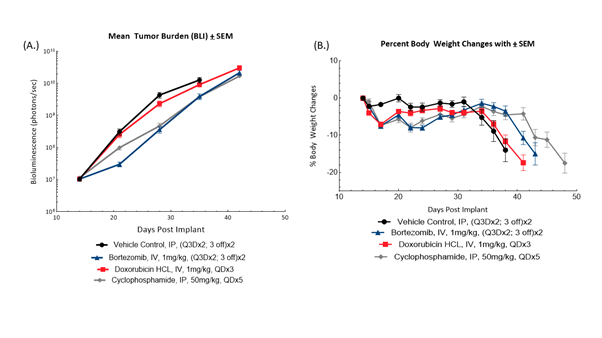
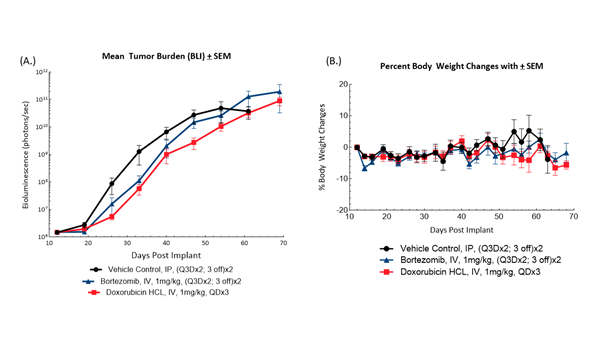
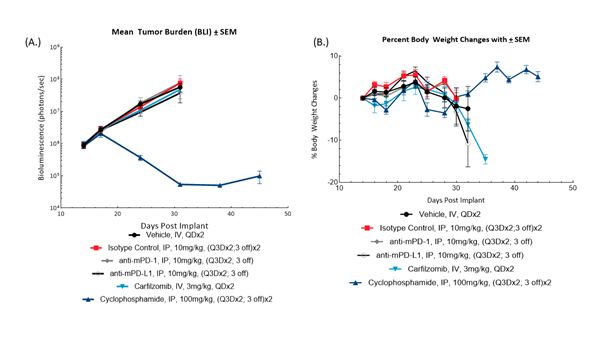
To understand the potential anti-tumor effects of novel therapeutics in combination with clinical standards of care, selection of the most appropriate preclinical tumor model is crucial. Human xenograft and mouse tumor models represent such a preclinical platform for evaluating novel test agents. At Labcorp Drug Development (formerly Covance Laboratories), we have a wide selection of tumor models for evaluating the efficacy and mechanism of action of test agents against multiple myeloma. MM1.S and NCI-H929 human multiple myeloma are two commonly used tumor cell lines grown in immunodeficient mice permissive of hosting human cells. 5TGM-1 is a multiple myeloma tumor line that was originally derived from mice, representing a syngeneic tumor model in which the host mouse has a fully competent immune system to evaluate immune-modulating agents. We have enabled these lines to express luciferase, an enzyme that produces bioluminescence in the presence of the substrate luciferin, in which light output can be measured as an indication of tumor burden and disease progression via bioluminescence imaging (BLI). These models are implanted into mice intravenously, disseminating the disease throughout the animal and producing bone lesions in a manner similar to clinical disease progression.
In these studies, we evaluate each model’s response to clinical standards of care, to characterize it as responsive (or refractory), so that our clients can select the most appropriate model for their program and identify opportunities for combination studies.